Lyle Nelson from the Congressional Budget Office (CBO) has been busy.
Two weeks ago, I commented on the results of Nelson’s review of 6 Medicare Care Management demonstration projects over the last decade. At the same time that report was released, Nelson also released a companion report on the 4 “Value-based Payment” CMS demonstrations over the same period. The following is my adaptation of the main results table in this new CBO report.

The most influential of these demonstrations was the Physician Group Practice Demonstration (PGP). The ten PGP participants included 2 faculty group practices within academic medical centers, 5 non-academic integrated delivery systems, one freestanding group practice, and one network consisting of 60 small practices. All had experience with care management programs before the demonstration, and all implemented care management programs in the Medicare population for the demonstration. These care management programs mostly consisted of nurses serving as care managers, focusing primarily on patient education and monitoring for patients with CHF or diabetes or meeting other “high risk” criteria. Most implemented chronic disease registries for use by the care managers, in addition to using electronic medical records systems that were already in place or in the process of being implemented before the start of the demonstration.
Two of the ten PGP participants received bonuses in the first year, since the Medicare expenditures were more than 2% below the expected expense. Four participants received bonuses in the second year, five in the third and fourth years, and four in the fifth year. A formal evaluation of the program conducted after the first two years concluded that the overall effectiveness of the PGP across the ten participants was about 1% gross savings in year two, and even lower in year one. Net savings, after counting the cost of the bonuses paid to some of the participants, was only 0.1% in year two.
The CBO report points out that even this meager 0.1% net savings might be an over-estimate, because PGP participants changed their diagnostic coding practices, making their populations appear to be sicker, and therefore making the risk-adjusted cost targets artificially high. Such revenue maximization efforts have been job one in Medicare Advantage plans for years. The PGP participants succeeded in lifting their risk scores by 8%, which was 3 percentage points higher than the increase in the comparison population. And, the savings might have been further overestimated because all four of the PGP participants that achieved reward payments in year two already had slower than normal growth in Medicare expenditures before the PGP demonstration began. All the other PGP participants that did not earn year 2 bonuses had pre-demonstration Medicare growth that was no different than the comparison population.
Despite these discouraging results, the PGP demonstration was nevertheless used as the main evidence base supporting the design of the Medicare Shared Savings Program, calling for the establishment of Accountable Care Organizations (ACOs). It is also the main evidence base for the associated Pioneer ACO program, for which 32 participating provider organizations have recently been selected.
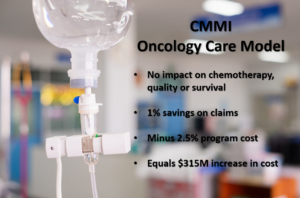
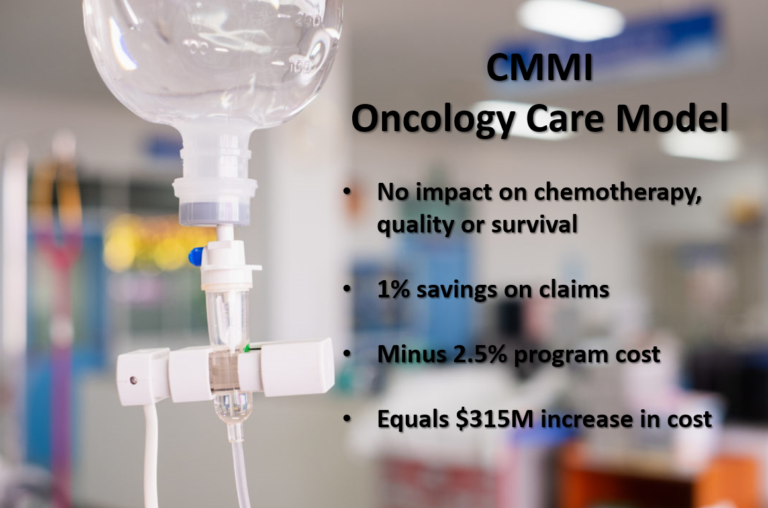
The Premier Hospital Quality Demonstration focused on 5 disease states and made bonus payments that amounted to only 0.25% of the total Medicare payments for those disease states. That’s two orders of magnitude less than the size of incentive payments thought to substantially influence performance. With such a tiny prize, it is not surprising that the quality improvements were assessed to have only a 1-5% incremental impact of process of care quality metrics during a period of time when such process of care metrics were improving nationally. And, the CBO report concluded that the demonstration had no effect on Medicare expenditures for inpatient hospital care. In fact, taking into consideration the reward payments, the demonstration led to an increase of costs by 0.3%.
The most successful of the demonstration projects was the Medicare Participating Heart Bypass Center Demonstration, which was used as a model for similar provisions in the health care reform law (PPACA). In this program, the hospitals negotiated their bundled payments up front, ensuring that Medicare received savings compared to typical fee-for-service cases. Overall, the program saved Medicare 10%.

So, where did the savings come from?
It’s possible that they just came from good negotiating by CMS with hospitals that wanted to get out in front of what they saw was an inevitable trend toward bundled payment. But, let’s assume that the hospitals really had a plan to reduce their costs in proportion to the negotiated decline in their revenue.
In interviews with leaders of the participating hospitals, the important changes in their approaches to patient management that were intended to reduce their costs included:
- Greater involvement by surgeons in postoperative care
- Earlier discharge of patients from the intensive care unit
- Greater standardization of surgical protocols and supplies
- Substitution of less expensive drugs for more costly ones, and
- Greater reliance on clinical nurse specialists for managing patients’ care in the hospital.
The participating hospitals substantially decreased their length of stay during the demonstration period, although length of stay for bypass surgery was dramatically decreasing nationally during that same time period.
However, probably more important than these process changes was the fact that all the participating hospitals created a physician reimbursement approach that established a fixed per case payment expected to cover all physician payments. This amount was split in defined percentages among the four types of specialists involved in every bypass case — the thoracic surgeon, cardiologist, anesthesiologist, and radiologist. Any payments to other specialists was essentially payed from this pool, reducing the payments to the four core specialties. Therefore, the hospitals created a strong incentive for the core specialties to limit referrals to other specialists. This undoubtedly led to a reduction in utilization of those other specialists and the tests and procedures they generate. Therefore, some of the savings probably came from reducing revenue to non-core specialists.
My conclusions
- Don’t bother with incentives unless they are large enough to change behavior. A 0.1% reward can’t work. Nor can a 1% reward. Try 10-20%.
- Don’t create asymmetrical up-side only incentives. They are far weaker in terms of motivating change. And, they create a problem with paying out undeserved rewards for lucky good results.
- Negotiate the savings up front, rather than just creating a game from which savings might be achieved.